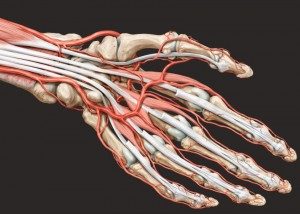
The hand is a complicated anatomic masterpiece that is responsible for grasping things, as well as for normal survival.
It is comprised of bones, tendons and muscles as well as nerves and blood vessels. Due to the continuous use of the hand in daily activities, it makes it susceptible to injuries or degenerative deteriorations.
Injuries usually involve the ripping of tendons and the fractures, whereas degenerative deteriorations present various forms of tendonitis and trapped nerves.
Trigger finger is the pathological condition in which a finger is bent because of the tendon. Movement results in pain and even a locked finger which remains in a bent position
This happens because the sheath (case) and the tendon swell and inflame, making the passage way narrower than normal causing friction on the particular tendon. In addition, a microscopic nodule can be formed on the tendon causing blocking of movement.
Its cause is still unknown and it usually affects women between 40-60 years of age. Predisposition factors can be diabetes and rheumatoid conditions.
The treatment always results in surgery which aims to open the ligament that causes the narrowing and then unblock it. It takes place in an operation room with local anaesthesia. The patient is able to return home the same day and from the next day the finger can be moved. Pain relief is immediate and recovery is very quick.
Conservative treatment includes anti-inflammatory medicine, rest and immobilisation. Occasionally a cortisone injection around the tendon is administered with satisfactory results.
There are other relevant conditions that are called stenosing tenosynovitis. One such condition is De Quervain tenosynovitis, which occurs on the outer surface of the wrist.

In the area of the wrist, more specifically the base of the thumb, a pair of tendons is routed, which surrounded by a case called a sheath.
When this area is inflamed, due to various reasons, it results in friction between the tendons within the sheath causing pain during movement of the thumb as well as when attempting to grip something.
Usual causes are excessive use of the tendons as well as rheumatoid conditions.
An orthopaedic surgeon can identify the condition by putting the patient’s hand through specific tests, without the need for imaging equipment.
In the beginning, conservative treatment is used with the aid of a cast and anti-inflammatory medication. Should this fail, the solution is a surgical operation.
It can be performed with local anaesthesia, under surgery conditions. A small incision allows the Surgeon to gain access and correct the narrowed tissue that causes the problem.
Results are immediate and recovery is very quick.

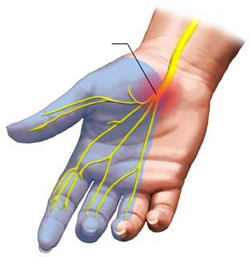
Carpal tunnel syndrome is a condition in the area of the wrist.
It concerns a nerve – the median nerve – which becomes pressed or squeezed at the wrist as a result of internal pressure and causes tingling and numbness of the patient’s fingers.
It was once thought that it mainly affected labourers, but recent studies have proven the opposite.
It affects people aged 25-65 and is more frequent in women. In addition, it can appear during pregnancy and it is considered temporary as it stems from swelling.
The largest percentage of cases are idiopathic, in other words without any real cause.
A less frequent cause is after a fracture of the radius (immediate pressure of the nerve from the bone or a hematoma in the area of the wrist)
It should be noted that any numbness of the fingers ought to be thoroughly examined by an orthopaedic surgeon using a detailed clinical examination that includes the patient’s history and the appropriate tests in order to exclude a possible neurological condition, which can present with the same symptoms.
The symptoms are numbness of the fingers such as the thumb, the pointer, the middle finger and half of the ring finger. Patients complain of numbness through the night and feel the need to put their hand out of the bedclothes.
The treatment can be either conservative or surgical. In the very early stages a cast could offer the patient some relief. In an advanced stage the solution is a surgical operation. After local anaesthesia, through a small incision on the wrist the trapped nerve is decompressed. After stitching the incision the patient returns home and protects the operated hand for about 10 days.
It is recommended that sufferers of this condition should not let it reach the final stages of this syndrome because the hand muscles can develop atrophy, making recovery long and uncertain.